The inguinal canal carries the spermatic vessels and cord in the male and the round ligament of the uterus in the female.
Going from the inside of the abdomen out in the region of the inguinal canal one would pass through;
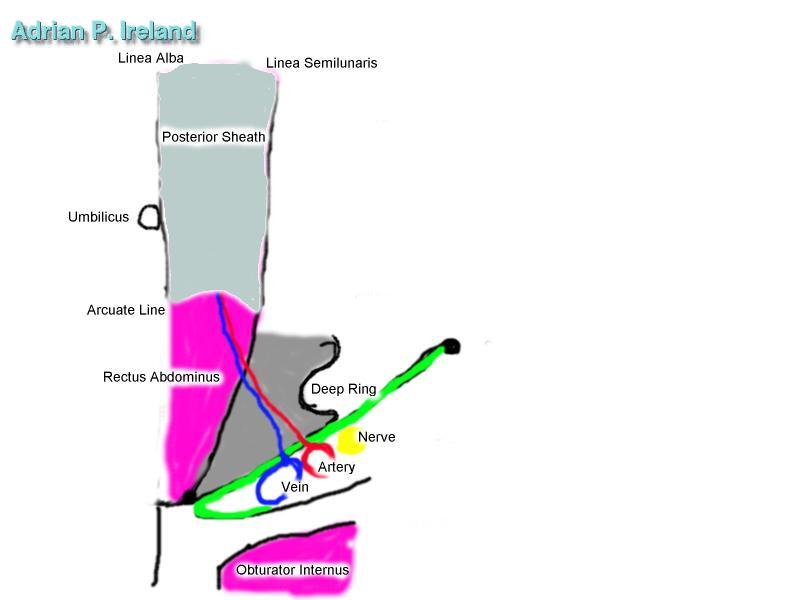
The canal may be viewed as the space through which the contents of the canal pass. It begins at the deep ring and ends at the superficial ring. A sack of peritoneum continues into the canal and is termed the processus vaginalus; an extension of this surrounds the testes as the tunica vaginalis. Some fat from the extraperitoneal fat may be seen in the inguinal canal; if this is large it is termed a lipoma of the cord. The testicular arteries and veins travel through the retroperitoneum to the deep ring; at that location the artery is surrounded by several small veins, this is termed the pampiniform plexus. The vas deferens arises out of the pelvis from the seminal vesicle to enter the medial side of the deep ring, it runs beside the pampiniform plexus. Both the pampiniform plexus and vas are surrounded by the internal spermatic fascia and cremesteric muscle and fascia in the inguinal canal; beyond the superficial ring they are also surrounded by the external spermatic fascia (from the aponeusoris of external oblique). The transversalis fascia and the transversus abdominus contribute to the internal spermatic fascia, which continues through the superficial ring into the scrotum. The internal oblique forms the cremesteric muscle; this gives an attenuated layer which conintues outside the canal at the superficial ring. The ileoinguinal nerve usually runs ontop of and in the creamester muscle and leave the inguinal canal at the superficial ring. A small arterial branch arises from the inferior epigastric artery close to the deep ring, it supplies the cremesteric muscle and enters it from the lowermost part of the muscle at the junction of the cremester and the inguinal ligament. This artery may act as collatoral blood supply to the testes if the testicular artery is damaged. The external oblique is in anterior; at the superficial inguinal ring it continues as the external spermatic fascia over the cord.
The inferior part of the inguinal canal consists of the upturned end of the inguinal ligament. The superior part of the inguinal canal consists of the arching fibres of the internal oblique and transversus abdominus. The anterior wall of the inguinal canal consists of the external oblique aponeurosis. The posterior wall of the inguinal canal consists of; (laterally) the transversalis fascia over the inferior epigastric vessels and (medially) the transversalis fascia covered by the conjoined tendon of transversus abdominus and internal oblique, and the relected part (Colles ligament) of the inguinal ligament.
Besides the ileo-inguinal nerve the genital branch of the genito-femoral nerve passes through the canal.
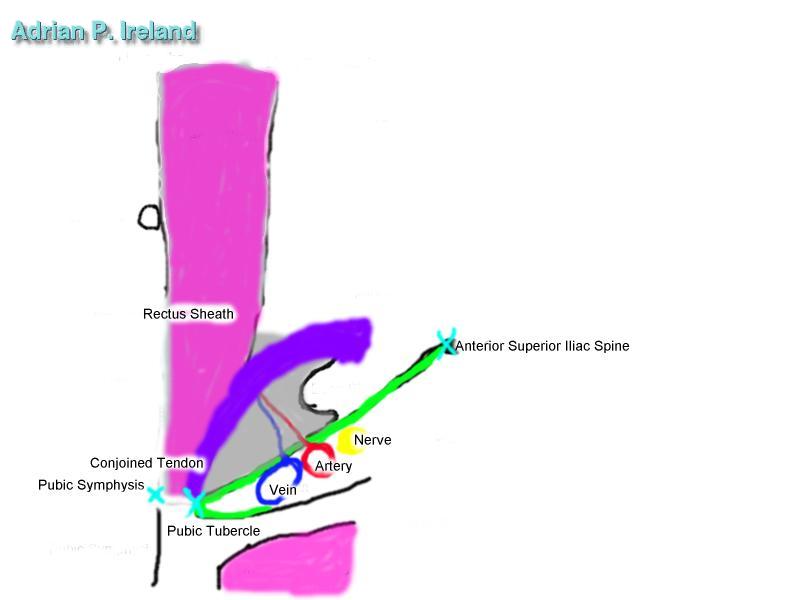
The anterior superior iliac spine can be located by tracing the iliac crest anteriorly untill the spine is felt as a protrusion at the palpable anterior extent of the crest. This is the lateral attachment of the inguinal ligament.
The pubic symphysis is where the two bones of the pelvis meet in the midline anteriorly. It may be located by running the finger in the midline downwards from below the umbilicus untill the bony pelvis is felt.
The Mid Inguinal Point is half way between the anterior superior iliac spine and the pubic symphysis. It is the landmark for the femoral artery.
The pubic tubercle lies about 2.5 cm from the midline and is difficult to palpate. Its position may be estimated by the point 2.5 cm lateral (horizontal line) to the pubic symphysis.
The Mid Point of the Inguinal Ligament is half way between the pubic tubercle and the anterior superior iliac spine. The deep Inguinal ring is located about 2.5 cm above the mid point of the inguinal ligament. The importance of this surface anatomy is that if the patient has a reducbile inguinal hernia, pressure over the deep ring should prevent the hernia coming out when the patient is asked to cough. Removal of the pressure and appearance of the hernia on coughing are confirmatory.