




Next: Barium Enema
Up: Investigation
Previous: Faecal Occult Blood (FOB)
Index
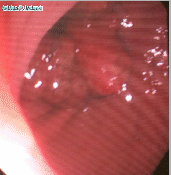
Figure 4:
Colonoscopic view showing recurrance of cancer at the site of an
anastamosis
 |
Colonoscopy is a useful investigation in the patient with suspected
colorectal cancer. It permits visualisation of the lining of the rectum
and colon and the terminal ileum. If suspicious areas are seen they may be
biopsied. Polyps may be removed for histological examination.
The colonoscope is a flexible tube about 2 m in length. The operator can
see what the end is looking at. Fibreoptics carry light from a light
source down the scope to the tip. The light reflects off the inside of the
bowel and is collected by a charge coupling device (CCD) integrated
circut. The information from the CCD chip is carried back up the scope to
be processed and displayed on a monitor. There are two wheels on the hand
piece of the scope and two buttons. The two wheels move the tip of the
scope back and forth and up and down respectively. Movement in either or
both of these axes can be reduced by a lock. One of the buttons (blue
button; blue is for BLOW) insufflates gas, it is a valve attached to a
pump with variable pressure, the other button (red button) is attached to
a vacuum pump for suction. The scope also carries a channel through which
the endoscopist can pass various instruments.
The advantages of colonoscopy are;
- Visualisation of the internal lining of the rectum, colon and
terminal ileum
- Possible to biopsy suspicious lesions for histological
conformiation
- Polyps may be removed
- Some theapeutic maneuvers are possible, (coagulation or
injection of bleeders, passing a balloon for dilation of strictures,
pass a guide wire to aid insertion of an expandible stent)
The disadvantages of colonoscopy are;
- Bowel preparation required, may cause cardiovascular affects in
susceptible patients
- Fasting required which makes management of diabetes difficult on
an outpatient basis
- Uncomfortable, unpleasent procedure that is performed under
concious sedation. The patient feels like they want to open their
bowels due to the sensation of the instrument being passed and the
insufflation of gas. Most patients are able to tolerate the procedure
or do not remember the procedure due to the effects of the drugs,
however, some find it too much of an ordeal and the procedure has to
be abandoned. Patient needs to be detained for a period after the
examination to ensure that they have recovered from the effects of the
drugs adminsitered
- Risk of adverse reaction to the drugs, or risk of over
medication, possible induction of seizures if reversal of sedation
required in epileptics
- Invasive procedure, with a risk of colon perforation, which may
prove lethal.
- Incomplete examinations, occur
- The operator may feel that he/she has completed the
examination when he/she has not. The anus is a reliable
landmark, but after that it becomes more difficult to be
sure where you are. There is thus the potential to miss
lesions in the distal bowel that has not been visualised and
the clinician is lulled into a false sense of security that
there is no problem when there may be.
- Poor bowel preparation
- Operator factors; the operator may not be skillful
enough to complete the examination. Even in the most skillful
hands the operator may not be able to do a complete
examination.
- Instrument factors; old instrument, too floppy, too
stiff, equimpment malfunction
- Patient factors; intolerance, tortuosity, pathology
encountered
Colonoscopy is the investigation of choice in a patient with altered bowel
habit or rectal bleeding who is suspected of having colo-rectal cancer. It
is also indicated;
investigation of lower abdominal and left iliac fossa pain,
screening for colo-rectal cancer in people with a strong family
history of colo-rectal cancer,
surveillence of the residual colon following resection for cancer,
investigation of anaemia (particulary if the FOB
test is positive),
disease follow up (polyps, stricture, Crohn's, ulcerative colitis),
diagnosis of patients with ischaemic colitis post aortic surgery,
diagnosis of Cl. difficle colitis,
colonoscopic de-rotation of sigmoid volvulus,
colonoscopic decompression of acute colonic pseudo-obstruction.
 Read more about:Acute colonic
pseudo-obstruction
Read more about:Acute colonic
pseudo-obstruction
Colonoscopy is contraindicated if the patient is suspected of having a
possible perforation in the colon or if a perforation may be easily
percipitated by insufflation of gas, for instance in suspected acute
diverticulitis and in patients with suspected large bowel obstruction.
Next: Barium Enema
Up: Investigation
Previous: Faecal Occult Blood (FOB)
Index
Adrian P. Ireland
